Benefits of TPN in critical care
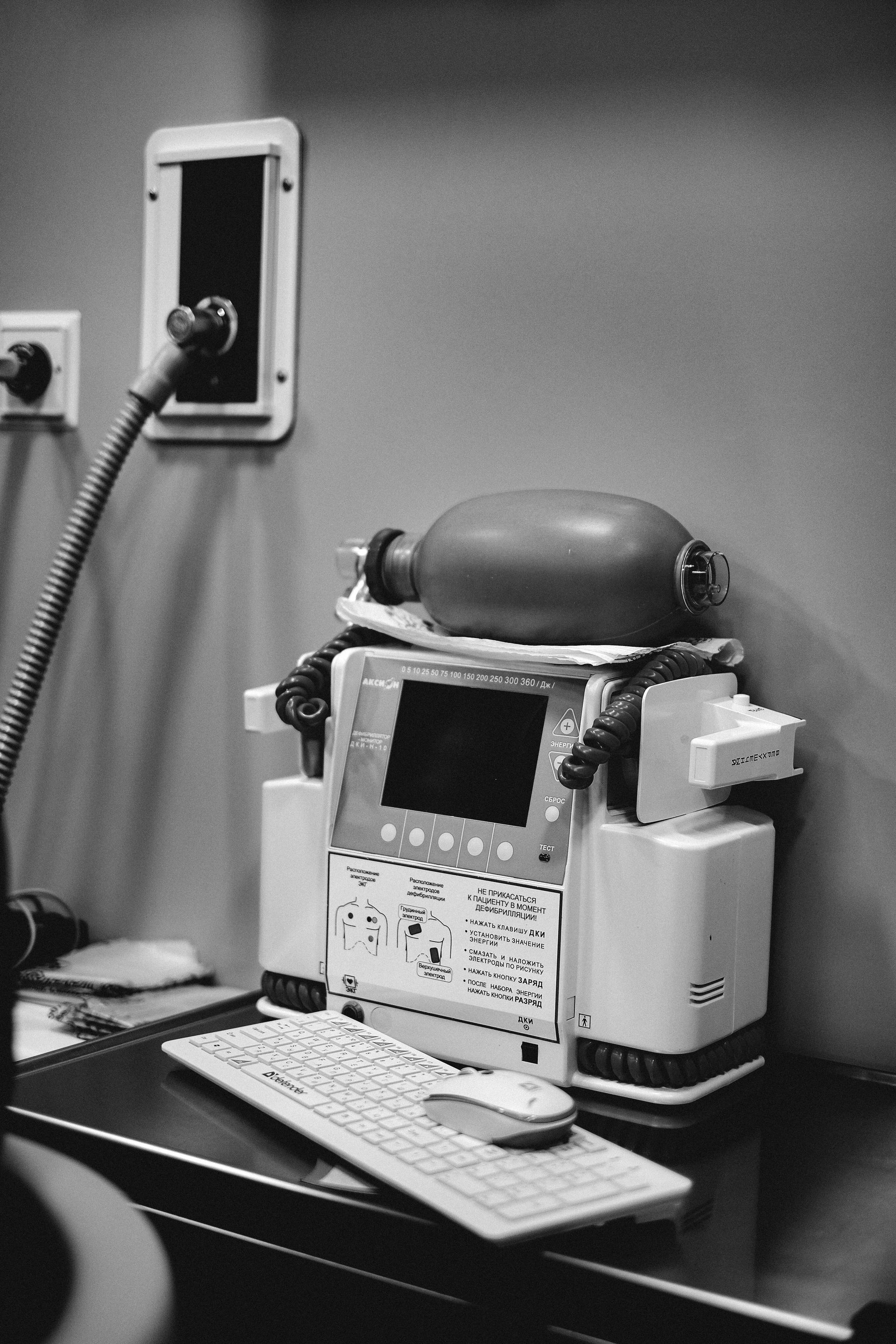
Total Parenteral Nutrition (TPN) plays a pivotal role in the management of critically ill patients. As a method of providing complete nutritional support intravenously, TPN becomes essential when the gastrointestinal tract cannot be used for enteral nutrition. While often compared to enteral feeding, TPN presents unique advantages in certain clinical scenarios. This article delves into the benefits, applications, and considerations of using TPN in critical care settings based on current evidence and clinical insights.
Addressing Malnutrition in Critical Care
Importance of managing malnutrition in critically ill patients
Malnutrition poses a significant risk to critically ill patients, with reports indicating that 20 to 40% may experience some form of malnutrition. This is particularly concerning in intensive care units (ICUs) where conditions such as protein-energy malnutrition can lead to severe complications. Addressing malnutrition is essential, as failure to do so increases both morbidity and mortality rates among this vulnerable population.
Prevalence and impact of protein-energy malnutrition
Protein-energy malnutrition is prevalent among critically ill patients, exacerbating existing health issues. Patients who are moderately to severely malnourished are at increased risk for compromised immunity, prolonged hospitalization, and adverse clinical outcomes. Enteral nutrition is preferred for most patients with functional gastrointestinal tracts; however, when enteral feeding is not tolerated or contraindicated, Total Parenteral Nutrition (TPN) becomes vital in meeting nutritional needs and supporting recovery.
Clinical significance of nutritional intervention
Nutritional interventions have a profound impact on recovery outcomes for critically ill patients. Guidelines recommend initiating parenteral nutrition within 3 to 7 days if enteral feeding is not feasible, particularly in patients with evident protein-energy malnutrition. Early intervention enables better caloric and protein intake, which is crucial for maintaining organ function and supporting tissue repair.
| Intervention Type | Nutritional Support | Clinical Outcome | Timing |
|---|---|---|---|
| Enteral Nutrition (EN) | Preferred | Reduced mortality, improved gut integrity | Early initiation recommended |
| Total Parenteral Nutrition (TPN) | Supplemental | Provides complete support when EN is inadequate | Initiate within 3-7 days |
| Early PN | Significant benefits | Lower 30-day mortality rates, better protein intake | Within 48 hours if needed |
Advantages of Total Parenteral Nutrition
Total Parenteral Nutrition (TPN) offers critical advantages for critically ill patients by providing complete nutritional support through intravenous administration, which is crucial when enteral nutrition is contraindicated or insufficient. It effectively addresses protein-energy malnutrition, commonly seen in these patients, which, if left untreated, can lead to severe complications such as muscle weakness, increased risk of infections, and delayed wound healing. TPN supports optimal organ function and recovery, particularly in hypercatabolic states like sepsis or major trauma, where elevated nutritional needs must be met. Properly managed TPN can reduce mortality rates and improve outcomes in patients with high nutritional risk, especially when initiated early. Monitorization is also vital to prevent complications such as refeeding syndrome and electrolyte imbalances, ensuring safe and effective nutrient delivery.
Clinical Applications of TPN
When to use TPN in critically ill patients
Total Parenteral Nutrition (TPN) plays a vital role in the management of critically ill patients who are unable to receive enteral nutrition. Conditions such as chronic intestinal obstruction, severe gastrointestinal dysfunction, or traumatic injuries often render enteral feeding unfeasible. In these scenarios, TPN ensures that patients receive crucial nutrients to prevent protein-energy malnutrition, which affects approximately 20 to 40% of critical care patients. Timely initiation of TPN, typically within 24 to 48 hours, is pivotal, especially for those exhibiting signs of malnutrition.
Conditions warranting TPN over enteral nutrition
TPN is indicated under various circumstances where enteral nutrition is unable to meet the nutritional needs of critically ill patients. Key conditions include:
- Bowel obstruction: When there is a blockage in the intestines, enteral feeding is not an option.
- Abdominal compartment syndrome: Increased pressure within the abdomen prevents effective enteral feeding.
- Severe pancreatitis: Patients often require bowel rest to manage this condition effectively.
- Gastrointestinal injury or surgery: Post-operative patients or those with severe GI complications may need alternative nutritional routes.
These situations highlight the importance of selecting TPN as a means to deliver essential nutrients safely when enteral methods are not advisable.
Nutritional support and organ function
The provision of TPN supports critical functions such as tissue repair, immune response, and energy maintenance. By delivering a precise macronutrient composition tailored to the patient's needs, TPN helps mitigate the adverse effects of malnutrition, including poor wound healing and compromised immunity. Research shows that appropriately managed TPN can significantly lower morbidity and mortality rates by promoting better overall recovery.
While TPN meets the nutritional needs effectively, it is essential to optimize care strategies such as careful monitoring of electrolyte balances, glucose levels, and signs of infection associated with the use of central venous catheters. By enhancing the oversight and quality of TPN administration, healthcare providers can minimize the associated risks and improve patient outcomes in critical care settings.
Evidence-Based Guidance on TPN
What does evidence-based guidance suggest about the use of TPN in managing malnutrition?
Evidence-based guidance clearly positions total parenteral nutrition (TPN) as a vital intervention for critically ill patients who are unable to receive adequate nutrition through oral or enteral means. This is particularly relevant in cases where gastrointestinal (GI) dysfunction occurs, leading to intestinal failure.
Guidelines for initiating TPN
TPN should be carefully considered after a thorough assessment of the patient’s nutritional status and individual needs. It's recommended to initiate TPN early, typically within 3 to 6 days for patients at apparent nutrition risk. This early intervention is crucial in combating the complications related to malnutrition and ensuring that nutritional requirements are met.
Factors influencing the initiation of TPN include:
- Severity of malnutrition: Evidence suggests that those exhibiting moderate to severe malnutrition derive substantial benefits from TPN.
- Inability to tolerate enteral feeding: Patients who cannot tolerate EN due to a compromised GI tract must receive TPN.
Monitoring and managing risks
While TPN is essential for nutritional management, it also comes with potential risks. Monitoring patients closely is necessary to prevent complications such as:
- Infection risks: Central venous catheters are prone to infection, which can be mitigated through improved catheter care and management practices.
- Metabolic imbalances: Regular checks for signs of refeeding syndrome and hyperglycemia are crucial, as high blood sugar levels can lead to increased risks of sepsis and mortality.
Strategies for minimizing complications include strict glucose control and using protocols to guide TPN administration.
Role of healthcare teams
The involvement of an organized and coordinated healthcare team is paramount when managing patients on TPN. Nutrition support teams play a key role in developing individualized feeding plans and monitoring patient progress. The American Society for Parenteral and Enteral Nutrition (ASPEN) guidelines emphasize a multidisciplinary approach to optimize outcomes, demonstrating the efficacy of teamwork in improving patient recovery while managing potential risks effectively.
In summary, while the role of TPN in nutritional management is critical, adhering to guidelines and maintaining oversight by healthcare teams ensures improved patient outcomes and reduced complications in critically ill populations.
Risks and Complications of TPN
What are the risks and complications associated with Total Parenteral Nutrition in critically ill patients?
Total Parenteral Nutrition (TPN) carries several risks and complications, particularly for critically ill patients. Some of the common issues include:
- Infection: Central venous catheters, often used for TPN delivery, can increase infection risk if not handled properly. In such patients, infections can lead to severe consequences, including sepsis.
- Metabolic Imbalances: TPN can result in metabolic disturbances such as hyperglycemia. Elevated blood glucose levels, especially over 180 mg/dL, can heighten morbidity and mortality.
- Refeeding Syndrome: For patients previously malnourished, restarting nutrition through TPN must be approached cautiously, as overzealous feeding can lead to metabolic disturbances, cardiac arrhythmias, and fluid overload.
Strategies to mitigate complications
To safely administer TPN and minimize complications, several strategies can be implemented:
- Strict Monitoring: Regular blood glucose monitoring and adjustment protocols should be in place to prevent hyperglycemia.
- Use of Care Bundles: Implementing best practices for central venous access can significantly reduce infection rates.
- Nutritional Protocols: Developing and adhering to TPN protocols with support from a multidisciplinary nutrition team can enhance patient outcomes.
- Alternative Lipid Solutions: Using new formulations and lipid emulsions may decrease the risk of metabolic complications associated with traditional TPN.
Importance of patient monitoring
Effective monitoring is paramount when administering TPN. Continuous oversight helps:
- Detect Early Complications: Rapid identification of issues such as catheter malfunctions or metabolic abnormalities allows for timely interventions.
- Adjust Nutritional Needs: Regular assessments ensure that nutritional needs are met without exceeding safe limits, promoting better recovery outcomes.
In conclusion, while TPN is often necessary for critically ill patients, its risks necessitate a careful, monitored approach. Effective strategies to mitigate these risks can help maximize the benefits of nutritional support and improve overall patient outcomes.
TPN vs. Enteral Nutrition: A Comparative Analysis
How does Total Parenteral Nutrition compare to enteral nutrition in terms of effectiveness and patient outcomes? [Comparison]
Total Parenteral Nutrition (TPN) and enteral nutrition (EN) present distinct differences in their effectiveness and outcomes in critically ill patients. Various studies underline that patients receiving enteral nutrition have enhanced survival rates compared to those on TPN. For instance, a notable study found a median survival of 317 days for those using enteral nutrition, against 195 days for TPN recipients (P = 0.017).
Enteral nutrition generally showcases lower rates of infectious complications. For example, the incidence of sepsis among TPN patients can be as high as 30.9%, compared to just 10.9% for those receiving enteral nutrition (P = 0.018). These stark contrasts suggest that EN can mitigate risks associated with infectious diseases while also promoting better overall health outcomes.
Effectiveness and patient outcomes
Beyond safety, enteral nutrition often results in decreased healthcare costs and reduced lengths of hospital stays. This economic advantage stems from its lower incidence of complications, such as those related to central catheters frequently seen with TPN. When patients can tolerate enteral feeding, it is endorsed as the preferred route for nutritional support.
While TPN may be necessary in certain extreme cases—such as bowel obstructions or conditions preventing enteral feeding—it does not replicate the beneficial effects of enteral nutrition on gut integrity and immune responses. Additionally, early enteral feeding has demonstrated reductions in infectious complications and improved clinical outcomes, further solidifying its preference over TPN.
Hospital care considerations
In hospital settings, effective management of nutrition is crucial. Around 20-40% of critically ill patients show signs of malnutrition, making timely and adequate nutritional support essential. Enteral nutrition provides significant health benefits, including maintaining gut integrity and preventing immune dysfunction, whereas TPN carries risks of hyperglycemia, which is a concern in critical care.
Overall, the choice between TPN and enteral nutrition should be guided by the patient's specific condition and tolerance. Enteral nutrition emerges as the safer, more effective option in most scenarios, whereas TPN should be reserved for cases where enteral access fails or is unfeasible. Thus, utilizing protocols and nutrition support teams can further enhance care quality in these patients.
| Nutritional Support | Median Survival (Days) | Sepsis Incidence (%) | Economic Considerations | Clinical Outcomes |
|---|---|---|---|---|
| Total Parenteral Nutrition (TPN) | 195 | 30.9 | Higher costs | Variable |
| Enteral Nutrition (EN) | 317 | 10.9 | Lower costs | Improved |
The Impact of Early Supplemental PN in Surgery
What impact does early supplemental parenteral nutrition have on mortality rates in surgical patients?
Early supplemental parenteral nutrition (PN) plays a significant role in improving survival rates among critically ill surgical patients, especially those who are at high risk of malnutrition. Research shows that initiating PN within 48 hours post-surgery can significantly reduce 30-day mortality rates. For instance, studies reveal a mortality rate of only 7.6% in patients receiving early PN, while those receiving standard care had a considerably higher rate of 26.7%.
In addition to lower 30-day mortality rates, the data indicates that in-hospital mortality decreased from 28.9% in the usual care group to 13.6% in the early PN group. This notable difference highlights the effectiveness of early nutritional support in critical settings where patients might struggle to meet their dietary needs due to their medical condition or surgical procedures.
Strategies for improved recovery
Implementing strategies to enhance early nutritional support can further promote recovery in surgical patients. While enteral nutrition (EN) remains the preferred method for feeding critically ill patients whenever possible, it’s not always feasible to meet optimal caloric and protein needs through this route alone. Studies have shown that the early PN group achieved caloric adequacy of 0.88 ± 0.34 compared to just 0.6 ± 0.29 in the usual care group, emphasizing the nutritional benefits of early PN.
Moreover, protein intake was significantly higher in the early PN group, with averages reaching 0.94 ± 0.39 g/kg compared to 0.47 ± 0.34 g/kg in usual care. This increased protein provision supports healing, organ function, and overall recovery in surgical patients.
Overall, while early PN presents a timely solution to combat malnutrition and boost recovery in the surgical ICU setting, careful consideration of individual patient needs and specific circumstances remains crucial to optimizing outcomes.
Optimizing the Timing and Dosage of TPN
Timing of TPN Initiation
Initiating Total Parenteral Nutrition (TPN) is a critical factor in the care of critically ill patients, particularly those showing signs of malnutrition. Guidelines suggest that TPN should be started within 3 to 7 days when enteral feeding (EN) is not feasible or tolerated. Early initiation is crucial for patients at risk of protein-energy malnutrition, as timely nutritional intervention can improve recovery outcomes.
Dosage Considerations
The dosage of TPN should be carefully optimized to match the patient’s energy needs, particularly to avoid hypercaloric feeding, which can lead to complications. Studies recommend tailoring caloric intake and protein levels to meet individual requirements, with a goal of providing at least 20% to 30% of caloric needs through EN when possible, thereby supporting immune function without compromising gastrointestinal integrity.
Nutritional Requirements
Accurately assessing nutritional needs through indirect calorimetry is essential, as traditional predictive equations may fall short in critically ill patients. Adequate protein and caloric provision are crucial during the patient's ICU stay to minimize the risk of adverse outcomes such as increased mortality. The emphasis on meeting nutritional goals highlights the importance of both timely initiation and proper dosage of TPN in critical care.
Monitoring and Managing Complications

Monitoring Strategies
Effective monitoring is essential in the management of parenteral nutrition (PN) to prevent complications. Regular assessments of blood glucose levels, liver function tests, and electrolyte balances are critical. The use of indirect calorimetry can provide accurate energy needs, ensuring patients receive adequate calories without risking hypercaloric feeding. This tailored approach to energy delivery helps mitigate the risks associated with PN.
Minimizing Complications
The aim of compassionate care is to achieve a 'near zero' complication rate with PN. Strategies include careful management of the central venous catheters, as many infections related to PN stem from catheter issues. Improving catheter care protocols can significantly reduce infection rates associated with PN, highlighting the importance of hygiene and skilled insertion techniques.
Role of Care Bundles
Organizational strategies, such as implementing care bundles for central venous access, are proven effective in minimizing complications. These bundles focus on standardizing practices around catheter care and nutrition delivery, ensuring comprehensive oversight. Additionally, involving nutrition support teams promotes adherence to protocols and enhances patient safety.
| Aspect | Importance | Best Practices |
|---|---|---|
| Monitoring Strategies | Essential for preventing morbidity | Regular glucose, liver, and electrolyte checks |
| Minimizing Complications | Reduces infection risk | Enhance catheter care protocols |
| Role of Care Bundles | Ensures consistent practices | Implement standardized care bundles |
Gastrointestinal Tolerance and Alternative Nutrition
Challenges with enteral feeding
Critically ill patients often experience gastrointestinal intolerance, which can impede enteral nutrition (EN) effectiveness. Factors like reduced gut motility and the presence of gastrointestinal complications contribute to this challenge. Under these circumstances, meeting caloric and protein needs becomes difficult, and patients may suffer from malnutrition, which can lead to serious health risks.
Role of TPN as an alternative
Total parenteral nutrition (TPN) proves essential for patients who cannot tolerate EN or when it is contraindicated. TPN delivers crucial nutrients, providing both essential and nonessential amino acids directly into the bloodstream. This nutritional support is vital for organ function and recovery. In scenarios such as bowel obstruction or severe abdominal conditions, TPN offers a lifesaving alternative to address nutritional deficits swiftly.
Balancing EN and TPN
While EN is preferred in most cases for maintaining gut integrity and reducing complication risks, a diversified approach that includes TPN can ensure that critically ill patients receive enough nutrition. Early initiation of nutritional support, whether through EN or supplementary TPN, aims to optimize recovery outcomes. Agencies recommend utilizing procedures and protocols to manage both nutritional methods effectively, leading to better patient care with a focus on balancing safety and efficacy.
The Historical Context of TPN in Intensive Care
Historical Development
Total Parenteral Nutrition (TPN) was pioneered in the 1960s, fundamentally changing the landscape of nutritional support in critically ill patients. Initially developed for patients with gastrointestinal disorders who could not tolerate oral or enteral feeding, TPN emerged as a critical intervention for those at risk of malnutrition, particularly within intensive care settings.
Clinical Studies and Findings
Research has consistently shown that malnutrition among critically ill patients is a pressing issue, with studies indicating that 20 to 40% of these patients exhibit signs of protein-energy malnutrition. Early studies demonstrated that proper nutritional support via TPN could indeed improve recovery outcomes, although newer studies suggest that early enteral nutrition should be prioritized. For example, a meta-analysis revealed that while both TPN and enteral nutrition were effective regarding survival, early enteral nutrition had the added benefit of fewer infectious complications.
Evolution of TPN Practices
Over the years, TPN practices have evolved, focusing on minimizing complications and optimizing nutritional delivery. The importance of proper management protocols and the involvement of nutrition support teams have emerged as crucial in reducing infection rates associated with central venous catheters— a common concern with TPN administration. Furthermore, advancements such as blood glucose control and alternative lipid emulsions have led to improved patient safety. The historical journey of TPN reflects ongoing efforts to balance the need for nutritional support with the imperative to minimize associated risks.
The Role of Nutrition Support Teams
Importance of Multidisciplinary Teams
Nutrition support teams (NSTs) play a pivotal role in the management of nutritional care for critically ill patients. Comprised of dietitians, physicians, pharmacists, and nurses, these teams ensure that each patient's unique nutritional needs are comprehensively addressed. Their collaborative approach enhances the assessment of malnutrition, optimization of nutritional interventions, and monitoring of treatment effectiveness, leading to improved patient outcomes.
Improving TPN Safety
The dire need for parenteral nutrition (PN) in cases where enteral nutrition is not feasible makes NSTs essential in minimizing associated risks. By employing protocols to streamline the administration of total parenteral nutrition (TPN) and regularly reviewing individual patient cases, NSTs can mitigate complications such as infections linked to central venous catheters. Optimizing glucose control and monitoring for signs of hyperglycemia also fall under their purview, helping to ensure safer delivery of nutritional support.
Patient Care Optimization
Furthermore, the involvement of NSTs in the early initiation of nutritional support—be it enteral or parenteral—facilitates timely interventions that can greatly improve clinical outcomes. Early nutritional support has been shown to prevent morbidity, reduce ICU length of stay, and boost recovery rates, underscoring the significance of these teams. In essence, the contribution of nutrition support teams is invaluable, enhancing both the safety and effectiveness of nutritional therapy in critically ill patients.
| Topic | Role of NSTs | Benefits |
|---|---|---|
| Multidisciplinary Approach | Comprehensive nutritional assessments | Improved patient outcomes |
| TPN Safety | Protocols for managing TPN | Reduced infection rates |
| Patient Care Optimization | Early initiation of nutrition support | Faster recovery and better survival rates |
Protocols and Guidelines for TPN Administration
Standard TPN protocols
The use of standardized Total Parenteral Nutrition (TPN) protocols is essential for managing critically ill patients. These protocols help ensure that patients receive all necessary essential and nonessential amino acids, vitamins, and minerals while preventing complications associated with TPN. Following established protocols assists healthcare providers in determining the appropriate nutritional composition tailored to individual patient needs, especially those who cannot tolerate enteral feeding.
Guidelines for safe administration
To minimize the risks associated with TPN, specific guidelines should be closely followed:
- Initiation Timing : TPN should commence within 3 to 7 days for patients diagnosed with protein-energy malnutrition when enteral feeding isn't feasible.
- Blood Glucose Monitoring : Keeping strict glucose control can alleviate the chances of hyperglycemia, thus lowering the risk of in-hospital infections and potentially improving recovery rates.
- Catheter Care : Proper management of central venous catheters is critical to reduce infection rates, as many complications often arise from catheter-related issues rather than TPN itself.
Impact on patient outcomes
Implementing structured TPN guidelines has been linked to improved clinical outcomes, including reduced complications and better nutritional adequacy. Studies suggest that patients receiving early and adequately managed TPN have lower mortality rates and improved recovery trajectories compared to those who do not receive adequate nutritional support. This highlights the crucial role of TPN in managing malnourished critically ill patients and the need for careful monitoring and protocol adherence.
TPN: Balancing Benefits and Risks
Assessing Risk-Benefit Ratio
Total parenteral nutrition (TPN) serves as a critical intervention for patients unable to consume or absorb adequate nutrition orally or through enteral feeding. While its deployment can prevent malnutrition—a significant concern as studies suggest that 20 to 40% of critically ill patients exhibit signs of malnutrition—TPN is not without risks. Hyperglycemia, infections related to central venous catheters, and the potential for liver complications are notable concerns requiring careful consideration in decision-making.
Clinical Decision-Making
In clinical settings, the decision to initiate TPN should be rooted in evidence-based guidelines. Recommendations suggest initiating TPN only after 3 to 7 days if enteral nutrition (EN) is not feasible, especially for patients with marked protein-energy malnutrition. Early intervention, particularly within the first 48 hours for high-risk patients, may yield improved nutritional outcomes. However, given the association between EN and lower complications, it is pivotal that clinicians weigh the urgency of nutritional needs against potential risks inherent to TPN administration.
Patient-Specific Considerations
Personalized care remains crucial in determining the appropriateness of TPN. Factors such as the patient’s medical history, nutritional status, and tolerance to enteral feeding inform decisions. For instance, critically ill surgical patients facing intra-abdominal complications may necessitate TPN to prevent severe nutritional deficits. Thus, establishing individualized feeding plans while considering both the benefits and risks associated with TPN is vital for optimizing recovery outcomes.
The Future of TPN in Critical Care

Emerging Trends in TPN Administration
The landscape of Total Parenteral Nutrition (TPN) in critical care is evolving through several key trends. As research continues to highlight the importance of individualizing nutritional support, more tailored approaches to TPN are being developed.
One notable trend is the increased incorporation of indirect calorimetry for assessing the energy needs of critically ill patients. This approach allows healthcare providers to avoid hypercaloric feeding by accurately determining individual caloric requirements.
Advancements in TPN Formulations
Advancements in the formulation of TPN solutions are also on the rise. The introduction of alternative lipid emulsions aims to reduce the risk of hyperglycemia and improve fatty acid profiles, enhancing overall patient outcomes.
Furthermore, the shift towards using structured protocols and the involvement of multidisciplinary nutrition support teams are strategies seen to potentially minimize complications associated with TPN, reinforcing its safe use in complex care settings.
Future Research Directions
Future research will likely focus on the long-term impacts of early versus late TPN initiation, exploring its effects on overall recovery and discharge rates among critically ill patients. Studies that compare the efficacy and safety of different TPN protocols can illuminate best practices moving forward. Moreover, understanding the relationship between TPN, gut function, and immune response in critically ill populations remains crucial for optimizing nutritional strategies.
Continued investigation into the risks and benefits of TPN can solidify its role in patient care, especially in scenarios where enteral nutrition is not feasible.
Cost-Effectiveness of TPN
Economic Considerations
The cost-effectiveness of Total Parenteral Nutrition (TPN) is a significant factor in critical care settings. TPN involves higher expenses due to specialized formulas, administration, and monitoring, which can strain hospital budgets. In contrast, Enteral Nutrition (EN) generally incurs lower costs because it requires less complex logistical support and fewer consumables.
Impact on Healthcare Budgets
Utilization of TPN can impact healthcare budgets dramatically. While it provides essential nutrition for patients unable to tolerate EN, the costs associated with TPN can escalate due to potential complications like infections from central venous catheters and extended hospital stays. These factors can lead to higher overall treatment costs, affecting the financial viability of critical care units.
Cost vs. Benefit Analysis
In evaluating TPN's cost-effectiveness, it's vital to conduct thorough cost vs. benefit analyses. While TPN is lifesaving for certain patients, particularly those who cannot receive EN, studies indicate that early enteral feeding reduces complications and potentially lowers overall costs. The benefits must be weighed against the financial implications, especially when patient survival and quality of care are at stake. Ultimately, optimizing nutritional strategies, including using EN as the first line, can enhance patient outcomes while maintaining economic sustainability.
The Crucial Role of TPN in Healthcare
Critical Importance in Patient Care
Total Parenteral Nutrition (TPN) is critical for critically ill patients unable to tolerate oral or enteral feeding. Malnutrition is prevalent in this population, affecting 20% to 40% of patients, which correlates with increased morbidity and mortality. TPN plays a vital role in ensuring these patients receive essential nutrients necessary for recovery.
Life-Saving Potential
In cases where enteral nutrition is contraindicated or inadequate, TPN becomes a lifesaving intervention. Research shows that early initiation of TPN can significantly improve caloric and protein intake, which is crucial for tissue repair and immune function. For patients with high malnutrition risk, early TPN can lead to lower mortality rates and improved overall outcomes.
Integration in Clinical Practice
To effectively incorporate TPN into clinical practice, adherence to protocols that emphasize early intervention and proper monitoring is essential. Optimizing timing and dosage can prevent potential complications, such as those related to central venous catheters. Moreover, partnerships with nutrition support teams enhance the safety and efficacy of TPN delivery.
| Topic | Importance | Key Remarks |
|---|---|---|
| Critical Importance | Addresses malnutrition in critically ill | Essential for recovery |
| Life-Saving Potential | Improved outcomes in high-risk patients | Reduces risk of mortality |
| Integration in Clinical Practice | Enhanced safety and effectiveness | Protocol adherence is key |
Concluding Thoughts on TPN in Critical Care
In summary, Total Parenteral Nutrition is a vital component in the management of critically ill patients, offering life-sustaining nutritional support when enteral feeding is not an option. While it presents numerous benefits, TPN also requires careful administration and monitoring to mitigate potential risks. Its role as an alternative feeding method highlights the importance of a well-rounded approach in nutritional therapy. As advancements continue in medical nutrition, TPN's application and efficacy in critical care are expected to evolve, improving patient outcomes and broadening its utilization.
References
- Parenteral Nutrition in the Critically Ill Patient - PMC
- Management of parenteral nutrition in critically ill patients
- Parenteral nutrition: never say never | Critical Care | Full Text
- Nutritional Intervention in Critical Care | Respiratory Therapy
- Enteral nutrition versus parenteral nutrition—the risks and ...
- Early supplemental parenteral nutrition is associated with ...
- Critical care nutrition
- Benefit of supplemental parenteral nutrition in the critically ill ...
- Parenteral Nutrition in the Critically Ill Patient - PMC
- Total Parenteral Nutrition - StatPearls